Blog
How Northeast Georgia Medical Center Improved Postpartum Hemorrhage Simulation with Avcath
When postpartum hemorrhage (PPH) happens in a rural setting, teams do not get a practice round. They get real blood loss, real minutes, and real consequences. That is exactly why Northeast Georgia Medical Center built a mobile simulation program designed to bring immersive obstetric emergency training directly to the communities that need it most.
But for years, simulating postpartum hemorrhage meant relying on complex manikins, improvised fluid setups, and workarounds that were difficult to reset and challenging to scale in a mobile environment.
Inside NGMC’s mobile program, one tool ultimately became the primary method used:
Tasha Murchison, MSN-Ed, RNC-OB, C-EFM, who helps lead obstetric simulation education tied to NGMC’s mobile simulation efforts, explained why she moved away from high-fidelity manikins and improvised bleeding setups:
“Avcath offers easy portability and requires less set up and clean up compared to high fidelity manikins.”
In a mobile unit where scenarios may run back-to-back throughout the day, limitations such as bulk, cleanup time, and workflow disruption were not sustainable.
This case study breaks down why Avcath became the default for postpartum hemorrhage training, how it supports realistic simulation with standardized patients, and why that shift matters for rural readiness across Georgia.
The Rural Reality in Georgia and the Need for Preparedness
Rural maternal health in Georgia faces structural challenges that directly affect emergency preparedness. Recent public health analyses report that rural counties can experience maternal mortality rates up to 2.5 times higher than urban areas, and that more than 60% of women in rural regions live over 30 minutes from a birthing hospital.
Georgia has also experienced ongoing rural access strain, including hospital closures and workforce pressures.
In obstetric emergencies, distance and time are not theoretical variables. They are critical factors.
Mobile simulation addresses that reality by bringing high-impact training directly to care teams in their own communities.
The old way of simulating PPH was a patchwork of compromises
Before adopting Avcath, Tasha used the same workaround many educators recognize: improvised fluid bags, food coloring, tubing, clamps, and constant instructor narration to explain to learners what they should be seeing.
When asked about her former setup, Tasha recalled:
“I used to get a thousand cc bag of saline, put food coloring in it… they’d open a clamp
to do the hemorrhage.”
While functional, this approach had limitations:
- Difficult to repeat continuously in a mobile setting
- Challenging to maintain realism while remaining clean and efficient
- Hard to run without breaking immersion
High-fidelity manikins did not resolve those issues.
As Tasha noted:
“I have veered away from using high fidelity manikins for postpartum hemorrhage because of the inability to utilize standardized patients, difficulty in transportation, and more complex clean‐up requirements.”
Why Avcath became the default for PPH training

Avcath did not just “improve” PPH simulation. It changed what was possible in a mobile, high-throughput training environment.
1) Rapid Reset and Repeatability
Mobile programs live on throughput. Tasha may run scenarios repeatedly across multiple groups in a day. Avcath fits that pace because prep is simple: fill the reservoir and run.
In her words:
“The Avcath…is amazing because I don’t have to perform several steps in order to do a postpartum hemorrhage. I turn it on, put it on the standardized patient, and go.”
2) Real-Time Visual Feedback Without Instructor Narration
In many simulation scenarios, instructors must verbally cue learners about what is happening. Avcath replaces that narration with visible, continuous blood loss. The continuous bleeding provides visual feedback that the intervention is incomplete, requiring
learners to continue escalation according to established postpartum hemorrhage response protocols. This is especially important in PPH because the clinical decision-making is time-bound and dynamic. Nationally, postpartum hemorrhage has been rising over time, increasing from 2.7% of delivery hospitalizations in 2000 to 4.3% in 2019 in a large U.S. trend analysis.
3) Simultaneous Interventions Under Pressure
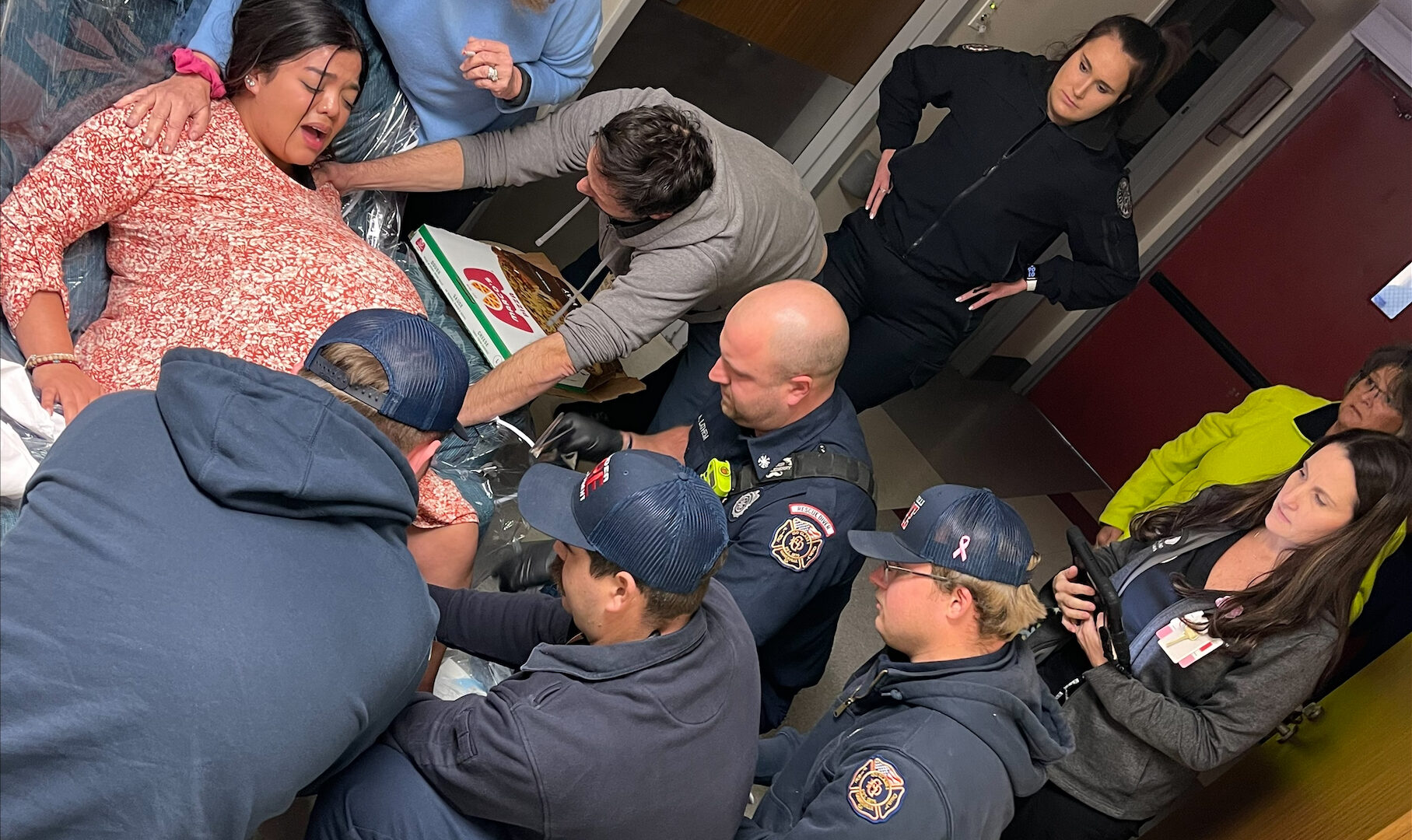
PPH response is not one skill at a time. It is simultaneous assessment and intervention. The system allows teams to perform simultaneous interventions, such as uterine fundal massage and urinary catheter placement, reflecting real obstetric workflow rather than isolated task rotation. That is much closer to real clinical workflow than taking turns with isolated task trainers.
4) Standardized Patient Interaction Enhances Behavioral Realism
A manikin can simulate vital signs. Standardized patients introduce fear, pain, urgency, and human interaction in ways that static equipment cannot fully replicate. Tasha’s key observation: with standardized patients, learners communicate differently, comfort differently, and behave more like a real OB team responding to a real person.
That matters for rural readiness because rural teams often must stabilize and manage longer before transfer is possible.
Preparedness You Can Drive to the Front Door
NGMC’s mobile simulation unit was built to increase access. Rather than requiring rural teams to travel for training, the program delivers simulation directly to their practice environment.
This aligns with broader rural simulation training goals documented by Georgia’s rural health organizations, including improving confidence, team communication, and preparedness where specialty resources may be hours away.
In a state where hemorrhage is recognized among pregnancy-related causes of death in public
health reporting, readiness is essential.
Avcath strengthens that readiness by letting rural-facing teams practice:
- Recognizing ongoing bleeding visually
- Coordinating parallel interventions
- Communicating with a live patient
- Executing response protocols without facilitator interruption
That is not “cool tech.” That is community resilience.




All photos are Courtesy of Northeast Georgia Health System
The Takeaway: Avcath Removed Barriers to Real-Time Learning
Avcath became the main tool over improvised setups and reduced the operational complexity of
prior methods used in the mobile program.
More importantly, it made high-quality, repeatable, realistic postpartum hemorrhage training
feasible at mobile-program scale.
As Tasha summarized:
“It’s a game changer.”
**Disclaimer: Avcath was invented and developed as a wearable Urinary Catheterization Simulator, not specifically for postpartum hemorrhage**