Blog
Determine the Right Modality Based on the Objective
Modality in healthcare simulation plays a crucial role in advancing medical education, training, and patient care. It refers to the various methods and tools used to replicate real-world healthcare scenarios, allowing healthcare professionals to practice, learn, and refine their skills in a safe and controlled environment. The importance of modality in healthcare simulation cannot be overstated, as it offers several significant benefits.

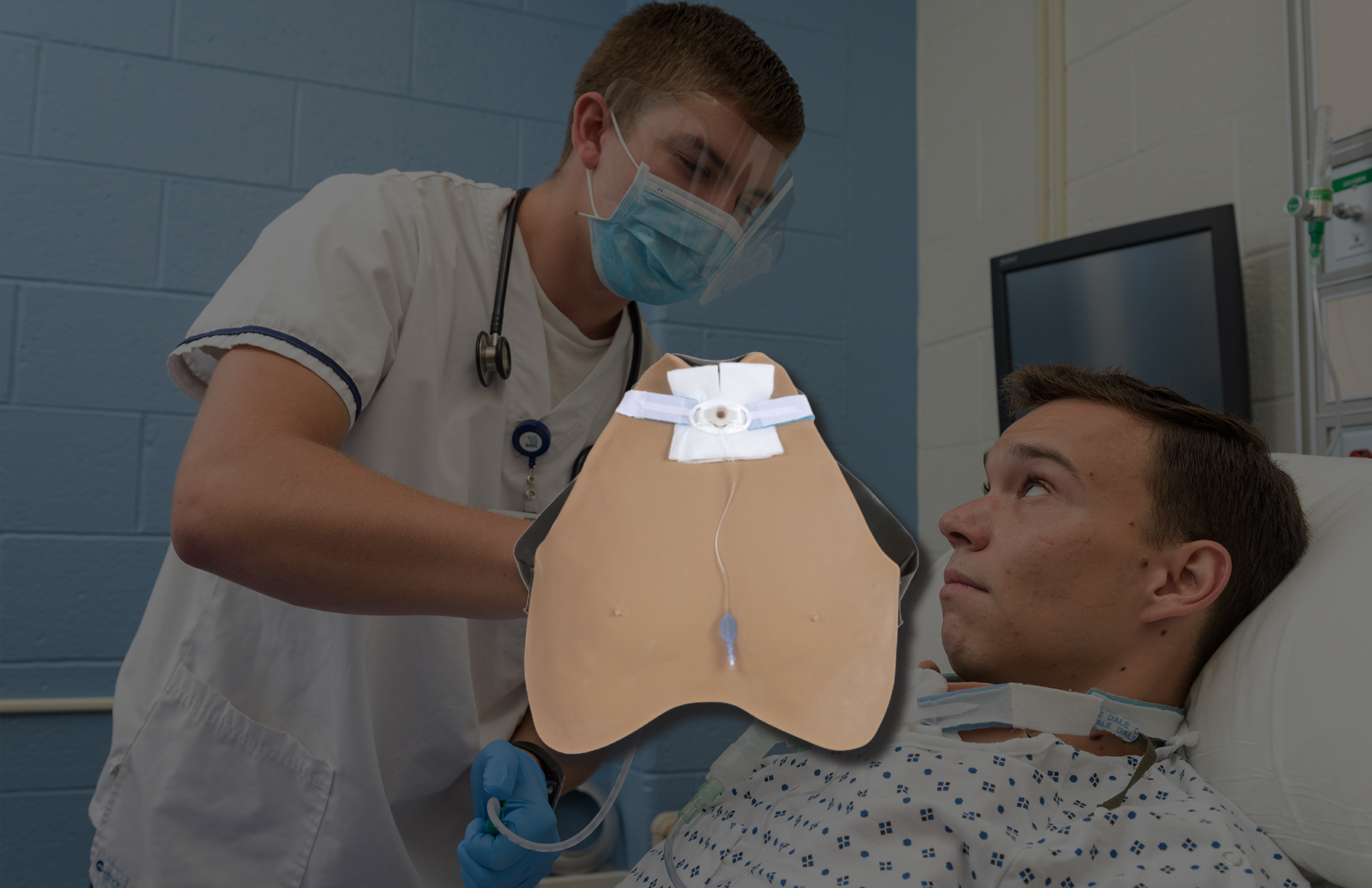
First and foremost, modality enhances the effectiveness of healthcare training and education. Simulations can encompass a wide range of modalities, including high-fidelity mannequins, computer-based simulations, virtual reality, standardized patients, and more. These modalities offer diverse learning experiences, catering to different learning styles and preferences. For instance, Standardized patients and wearable simulators allow for hands-on, realistic training, while virtual reality can create immersive scenarios for more complex procedures. This versatility in modalities ensures that healthcare professionals can receive tailored training that suits their needs and skill levels.
If you enjoyed our guide to The Right Modality Based on the Objective, check out more episodes of Simulation Nation below, and subscribe to our podcast and Youtube so you never miss an episode!
Full Transcript:
00;00;00;03 – 00;00;17;27
—-
This episode of Simulation Nation is brought to you by asking your one stop shop for everything wearable simulator and standardized patient.
00;00;18;00 – 00;00;59;29
—-
Hello, everybody, and welcome to the simulation nation. Today we are going to talk more about modalities and when to choose. Different modalities for your simulations. Yeah, and I think that, you know, a lot of people kind of Tenaa says the hybrid simulation with wearable simulators in ASPs, which is definitely where where our sweet spot is. But we have had experience with others or talked to a lot of people that are different using different modalities and just want to kind of share with you, you know, the kind of the from the body of information that we have to help you make better decisions as you are trying to decide what simulation is next and what are
00;00;59;29 – 00;01;20;01
—-
your objectives and then what modality is going to go along with that. As you design your sims. Yeah, and I think also just creative ways of being able to use different modalities. I think that there’s a lot of different concepts of how people have used hybrid simulation beyond just steer nice patients and attach trainers or eyes patients and wearable simulators.
00;01;20;03 – 00;01;51;12
—-
And I think that there’s a lot of different ways of being able to incorporate it that are very unique and creative to meet the objectives of the simulation. Yeah, and we did some really cool and creative things when we were doing simulation on a full time basis. So we can talk about those too. Yeah. So to start off, I go back to this conversation that I had a long, I guess it was a few years ago now, and I remember having a consultant who came up and she was working a lot with serious patients, and she started talking to me kind of about different modalities or different concepts.
00;01;51;14 – 00;02;15;04
—-
And she said, You know what are your thoughts? What are your feelings on these different modalities? And my response was, it was a test. Well, my response was that there’s a time and place, right? There’s a reason why these different modalities have come up. There’s different reasons why patients, you know, products are emerging into the market. And her response was, well, as a Syrian patient.
00;02;15;05 – 00;02;33;08
—-
Because, again, that’s my background. You don’t hate other modalities. And I was like, no, because standardized patients are not always going to be the solution. And I think sometimes the mindset is that that if you especially come from that background, then it’s like, well, it is the only answer. You design your arms around it. This is how you need to do it.
00;02;33;11 – 00;02;54;18
—-
And I think that there is a bad rap for Syrian eyes patients that they feel like their job is being is in danger by now, diversifying the modalities of simulation. And I would like to have it where everyone kind of has that open mind in terms of what are the best options for the objectives and for the simulations.
00;02;54;21 – 00;03;23;15
—-
You know, when you’re in that design concept. Yeah. And I mean, I think if you look at, like you said, there are things that have emerged in simulation since I started in 2006. Yeah. And they have come out of a need. We’re trying to fill a niche, right? You know, when we’re not, with all things considered, when you think about environmental fidelity and wanting to make this as closely applied to the clinical experience that they are going to have, there’s times and places for everything.
00;03;23;15 – 00;03;47;25
—-
Yeah. And I think it’s really important that as you you as you’re considering your simulations, you are including the fact that there is not it’s not a one size fits all. Yeah. As far as simulation goes. Yeah. And recently when we were talking at Camp Houston, when I did a presentation on the different modalities, how I equated it, I think that it’s a good analogy is just what are the tools in your tool belt?
00;03;47;28 – 00;04;08;26
—-
And some some centers are going to have a lot of tools and then tool belt and a lot of ways that they can use, you know, a lot of different creative ways. And some people are going to be more limited. They’re going to have more basic tools in their tool belt. And I think that the important part is simulation is we can get very creative with what the objectives are and making sure that the simulation has an environmental fidelity.
00;04;08;28 – 00;04;30;23
—-
But what I would caution a lot of people is if you don’t have the right tool in your tool belt, you might need to rethink that simulation before just being like, this is the same. I will make it work. You’re going to lack some of that environ environmental fidelity. And again, you’re probably then going to get feedback from your students about, you know, maybe some inconsistencies, maybe some trouble with that.
00;04;30;25 – 00;04;54;20
—-
And my suggestion would be, before you jump into that SIM, make sure you have the appropriate tools to be able to accomplish those objectives in that simulation the way you want it to. Yeah. And I think again, like when you say that, I think of the time that we had the meds in the room with, you know, for the sim the meds were like at the, at the sink area.
00;04;54;22 – 00;05;18;24
—-
And what we got feedback from the clinical instructors was that the students were taking the meds in clinical, now in the hospital setting and taking them into the room and leaving them there. And that’s just a you know, you’re not supposed to do that ever. So we were actually having to rethink how we how we had our meds, the accessibility of the meds, and were we reinforcing that, you know, are we using that same thing?
00;05;18;24 – 00;05;43;12
—-
So though that has nothing to do with modalities. It does have the did the same concept of that. You always have to be getting feedback from subject subject matter experts. And it doesn’t mean that you can’t hit the objectives with a different approach, but it does mean that you have to consider that in your design. Right. So one of my what I thought of when I was thinking about this was in past years.
00;05;43;14 – 00;06;20;19
—-
This was a long time ago. But when they were doing a maternity simulation and wanted to add in some people from diverse backgrounds. And the concept was, we’re going to have this mom have done cocaine before she came in the simulation. And at the time, they were only using mannequins for that sim. Well, I don’t know how like one plus one equal to like, I don’t know how they got to this place, but B, the concept was, we’ll just put some white powder under the mannequins nose, like on their upper lip to show that they had done cocaine before they came in.
00;06;20;26 – 00;06;46;22
—-
That’s how we’re going to meet that objective. And that, to me, is one of the biggest. Like they didn’t have the ability to have a standardized patient, someone in the room who could properly represent this patient, the physiological responses. But they also wanted to include this diversity element into the SIM so they didn’t have any other way of doing it other than something that really is not environment.
00;06;46;24 – 00;07;14;24
—-
Correct. You’re never going to. Well, I shouldn’t say never, but it’s highly unlikely anyone’s going to walk in and be birthing a baby with cocaine still in their nose. I mean, and I think the other caution to that is that furthering the stereotype sac where, you know, the students are expecting that if if they if they have no experience with this in their own personal lives, which probably most of them don’t, that that they’re going to walk in if somebody has been doing drugs, that there would be white powder under their nose, which leads people in the wrong direction.
00;07;14;25 – 00;07;38;01
—-
So what were your clues that this person was doing drugs? Well, they had white powder still under there. There are still residue there. That was my only indication to understand that the patient population we were trying to represent there. Right. But I think that those are the concepts of when simulation can go wrong in terms of that environmental fidelity or simply not using the tools that you have to create to meet the objectives that you’re trying to.
00;07;38;01 – 00;07;59;25
—-
And I think that we there’s it’s always going in with good intentions, but I do think sometimes we can get tunnel vision. And I think that in that simulation as mine, the mindset was I have a mannequin, I want to include this as the objective. How do I get there? All right. That’s how I get there. And rather than bringing in subject matter, experts are people who are objective into the scenario to say, is this a good idea?
00;08;00;03 – 00;08;22;26
—-
Well, I think sometimes we just keep moving forward. Yeah. And I think again, from the mindset of a simulation as it’s in that situation and it wasn’t me, so I can’t speak to it. I’m an air nurse. I am not anything maternal child whatsoever. But you do the best you can with what you have, and sometimes you’re just being asked to accept that this is the only tool in your tool belt.
00;08;22;28 – 00;08;46;26
—-
And so you do your best. But in some situations, like I said, it can lead to being misleading. So yeah, so let’s talk for a second about do you want to start with past trainers and kind of move our way up? Sure. Okay. So we actually wrote Aid in defining excellence in simulation. The second version, we allow them to volume to know is a volume to net.
00;08;46;26 – 00;09;09;16
—-
It would be a publication to whatever publication I call it, Volume two, like they asked us to write a chapter on task trainers. So we started with really kind of the static, you know, task trainers that are typically used in skills and simulation and worked our way up because there are, you know, they become more sophisticated. Unfortunately, in our opinion.
00;09;09;16 – 00;09;38;00
—-
They didn’t have a whole chapter on wearable simulators, but we were able to really define out the difference between adding technology into these body parts that, you know, really make the authenticity and the physiology appropriate. So from the perspective of task trainers, what were some of the things that you talked about in your presentation at Sam Houston? So we discussed more in terms of using them for a hybrid concept inside of simulation.
00;09;38;07 – 00;09;58;06
—-
So we’re not really going to touch too much on skills just because I think that then that opens up a whole nother avenue to discuss. But in terms of simulation, being able to use it where it could potentially be on a table where students are moved over from, you know, the mannequin or this nice patient over to a table top to complete the skill that that they’re expected to do during STEM.
00;09;58;06 – 00;10;20;01
—-
So either that starting an I.V., it could be doing, you know, a suture, you know, whatever it is or the concept of actually having it where it is in bed with that mannequin or the Syrian ice patient to almost act as an additional, you know, their height, one limb to make the new arm that like put it inside the hospital gown or something.
00;10;20;01 – 00;10;41;12
—-
Yeah. Do kind of to try to like mitigate that. And I think the main benefits with that number one is it’s cost effective. So being able to use various tabs traders inside of simulation, it definitely helps with being able to maintain some of the wear and tear that can come with mannequins in terms of, you know, sticking with IVs or needing to get them re skin things along those lines.
00;10;41;12 – 00;11;02;06
—-
It does help with kind of that logistical purpose. It also does help in terms of setup and take down because needing to put the fluid X inside of the mannequin and be refilling those fluid acts, especially if you think about like urinary catheterization and things like that. It is not an easy process to go back in and keep refilling that, especially when you have a lot of students going through.
00;11;02;12 – 00;11;25;29
—-
And in SEM, typically they are like draining the full bladder. So then you have to go back in and put in a whole nother well amount of, if I’m honest. The problem with that, with with mannequins we’re putting in the urinary Catherine is because there’s no pressure on the bladder, the catheter goes in and then because it’s it’s rubber, it essentially floats to the top.
00;11;26;01 – 00;11;44;21
—-
And then you also you only get a small amount of urine, feel like maybe 100 ccs. But if you wanted to actually put 400 milliliters in to the to the bag of urine so they could see that, hey, there was some urinary retention or yeah, you know, they did a bladder scan and you know that. So all of those things, there’s limitations within that.
00;11;44;24 – 00;12;03;01
—-
But it does help when you have the tap strainer to just again, reduce the need for needing to go in and reset that every single. So that typically without tap strainer it’s going to be a lot easier to just kind of because they are they’re built for skills right They’re built for repeated so usually set up and take down to a little bit easier and quicker to refill.
00;12;03;03 – 00;12;24;23
—-
The biggest drawback in terms of incorporating strainers in the simulation is just that environmental fidelity. I think that you’re just always going to struggle when you are taking the students out of the scenario they’re in to move them over to a tabletop. It’s just not going to flow the way of an authentic interaction, right? Is going to feel choppy.
00;12;24;25 – 00;12;50;13
—-
I think that sometimes it can be done well in terms of moving them over and that being built into the flow of the stem. But I think that we all know that being able to just have it kind of run full through is always going to be the ideal versus having to break that up. And then also, even if you do have that chance to enter in the bed with the mannequin or the super nice patient, there are a lot of things that can go wrong.
00;12;50;15 – 00;13;10;18
—-
I remember specifically we did one with the IVR and it was just super awkward in terms of it wasn’t connected to anything. So that was the challenge, was that it was just very free floating. So being the serious patient in the bed and again my arms behind my back to feel like this is my new arm, it just there’s no can.
00;13;10;18 – 00;13;24;27
—-
It’s not actually connected to my shoulder. So it’s just kind of again, it can be manipulated, it can be moved. My greatest fear was it just falling out of bed and having to be like happened a few times? It’s all it’s all the floor now, You know, that was my biggest fear was like, how do you come back from that?
00;13;24;27 – 00;13;48;18
—-
Because when those things happen too, then kind of like remain in character and be this serious person. Yeah, makes it very challenging because it’s clearly a funny situation. And so then to expect that students wouldn’t laugh or would, you know, come out of that, I don’t think it’s realistic to think that they look of any any goodwill, even even if they’re trying to remain engaged.
00;13;48;18 – 00;14;13;10
—-
That’s a funny thing to have to overlook. And what’s that? Comedian’s name? Nurse. Nurse Blake. And there’s Blake. Like, if you watch some of his parodies, like, it reminds you a lot of what You know what? Can’t go wrong in terms of environmental fidelity. Yeah, And, like, especially when the Ivy one comes up, Especially if you don’t have a semtech because they’re worried about putting fluids into the mannequins and things along those lines.
00;14;13;15 – 00;14;37;26
—-
Skinning them is really hard, but at least it has been historically. Yeah. And so it is something where they’re going to choose that option over having having them, you know, start an Ivy and infused. Yeah. It’s, you know, there’s all kinds especially in medical school and stuff, They’ll have them put in central lines and things. The other thing I would say to that is that it requires a really advanced ESP to be able to react to what’s happening.
00;14;37;26 – 00;15;14;24
—-
As far as procedurally. Yes. You know, if you think of a speed, it’s fairly new to the to the circuit. That may be too much to expect them to be asking questions and interacting because they don’t really know what they’re feeling. They don’t really have a well, because you’re not actually seen. I remember when we did one that I think it was removing tag a term from the Ivy Farm, and when they were doing it, it was so weird because you are reacting, but like you’re watching it, like you’re it’s isn’t your natural human instinct is that you’re not going to necessarily be watching someone take it, take it, or else if you’re in pain,
00;15;14;24 – 00;15;32;25
—-
you’re that hurts. You know, But you had to watch to see when they’d be ripping it because you needed to know when you actually supposed to be in pain. And so, like that just makes it like an uncomfortable situation where you’re trying to make it realistic, but it’s clearly not realistic to what’s going on. Yeah, Yeah, exactly. Yeah, I agree with that.
00;15;32;25 – 00;15;52;17
—-
And I think that that is a different element that I hadn’t thought of. But it is true that that reaction and response to the care being provided, especially in terms of urinary catheterization and things like that, if you are putting attached trainers and expecting them to react to respond, you have no idea what’s happening. So again, you’re doing your best, but you have no concept.
00;15;52;17 – 00;16;10;22
—-
Hence why there are sensors inside. Yeah, but you’re really you’re really trying to work off of the things they’re saying versus right. Being able to do it any other way. Right. And I think that serious patients really do appreciate being able to have other elements a part of the session. Like I think they enjoy having something they like to challenge.
00;16;11;10 – 00;16;37;09
—-
But I do think that there are a lot of additional elements that come into it for that environmental fidelity, for it to feel like a fluid process, you know, to make it realistic. So then moving on, do you want to move on to mannequins or on to VR? Yeah, I mean, one one story that I wanted to talk about with the mannequins was when we did the Code Blue simulation where we had an ASP that was having active chest pain.
00;16;37;11 – 00;16;59;18
—-
And when the nitroglycerin was administered, the ASP, that was ASPs cue to go unconscious. And they knew from the pre briefing that they were going to move over to the mannequin for the remainder of the simulation. So that’s another form of hybrid, right? It’s including ASPs and mannequin simulation. So you can also think about that if that if it’s an appropriate thing to do.
00;16;59;18 – 00;17;23;07
—-
We we’ve I’ve done it where it’s a code situation a couple of different times. But you know when you think about hybrid, that that’s another option. A hybrid is simply just combining two different modalities to make it more environmentally in the environmental fidelity to be more so. Yeah. So let’s go into mannequin based. So anything with mannequins, that is the accepted modality.
00;17;23;07 – 00;17;48;05
—-
I think that that is the way it’s used. Obviously with the earliest adaptation of what we are in the U.S. simulation in countries like the UK and Australia. Actually ASPs was the first modality and OEM’s they do. They’ve been using ASPs for forever. But I think that concept of using mannequins is what predominantly people are comfortable with. I think that that’s the normal situation and I think that people are beginning to diversify with what kind of tools they want in their tool belt.
00;17;48;12 – 00;18;05;13
—-
I do think that it’s hard in terms of looking at mannequins because there is such a wide range, like if you are looking at the lower technology to the higher technology, I don’t like to use the term low fidelity, high fidelity, because I think that that is not the correct term is that having more technology means more fidelity.
00;18;05;13 – 00;18;27;28
—-
I think that that is a term that very creatively in marketing that was coined by the mannequin companies. So I like to consider it more technology based and fidelity based, and that’s in the literature too, that’s coming out more recently too. Again, with this emphasis on fidelity and really kind of reclaiming that term. But I think that there is a wide range in terms of the lower technology mannequins.
00;18;28;04 – 00;18;56;10
—-
I mean, those are what we typically would use in skills. It’s very challenging to use those low technology mannequins in simulation in general, especially if there are not other modalities being incorporated into that simulation for those mid-level mannequins. I think that being able to have them in SIM is I think you can absolutely use them based off of the needs that you have inside of your objectives, in your simulations and things like that.
00;18;56;16 – 00;19;17;26
—-
And then the higher technology mannequins. I think for nursing SEM can often be too much technology for what is needed. I think that a lot of times there’s a lot of additional components that aren’t necessarily essential to meet the objectives of the simulation. And I think that’s been a common feedback that especially for undergrad, I should specify undergrad nursing.
00;19;17;27 – 00;19;42;05
—-
Yeah, I mean, I think that was common to back and that’s why the mid mid fidelity or mid technology technology programs came out right, or mannequins came out is because there was times where you felt like you were paying for all of these additional feature functions that you did not need. But unless you had like a C.R. in a program or you had, you know, you were doing anesthesia, it wasn’t necessary.
00;19;42;05 – 00;20;10;15
—-
But again, the early inception of this really went back to the whole idea of anesthesia. Anesthesia right. So the way that the way that the CAC mannequin was initially set up was always based on the physiology. And then with simian to anesthesiologist created this difficult airway. They were from University of Pittsburgh and they were trying to find a company to produce it.
00;20;10;15 – 00;20;37;02
—-
Yeah. And one of our board members, actually, David Broussard, his wife, he worked for Medical Plastics Technologies, Inc., and his wife had to have emergency appendectomy and had a difficult airway. And the surgeon told him or the nurses geologist, but I told him but basically said, your wife has a very difficult airway. So if she ever has to go for emergency surgery, make sure that you are telling them that she has a difficult airway.
00;20;37;05 – 00;21;08;22
—-
Well, so he was trying to find when when they approached him about getting this incorporated, he was all for it because he had a personal experience. Right now, they and Laird all ended up buying medical technologies or medical plastics, whatever it was, but layered on to buying them so that everyone knows it is a little mannequin. But so actually both of those mannequins came out of the idea of anesthesiology, intubation, you know, that kind of thing.
00;21;08;22 – 00;21;30;05
—-
So so that you can see where that’s all you have to have a high fidelity piece to to really be practicing knowledge piece. Sorry, high technology piece. I am definitely soaked in in the in the insight industry. But you have to have that you have to have a lot of technology in that to be able to do that in general type things.
00;21;30;11 – 00;21;52;19
—-
So as nurses, we felt as though we don’t need all of this, especially in undergraduate, which is where I focus most of my time. I don’t need all of these things. I don’t need difficult airway, right? I don’t need it to be able to, you know, attach to a ventilator or anything like that. And so that’s where really kind of the inception of this mid fidelity mannequin came out on the under the market.
00;21;52;19 – 00;22;17;28
—-
But but just know that from the beginning that’s why it was yeah. The all the bells and whistles and I can understand why they would start with that and based off of kind of historic historic knowledge. But the as they moved forward, they came out with this to make it a little bit more palatable as far as price because we didn’t have to now we didn’t have to pay for, you know, all the different teacher functions, but required the higher technology.
00;22;18;03 – 00;22;34;28
—-
Yeah. And I think that oftentimes people will see it as, you know, when we’re doing presentations, talking about things that in any type of way we are bashing mannequins and I want to be very clear that there are time and places for mannequins. I think what our soapbox are, what we’re preaching, is there’s other ways to do it.
00;22;34;28 – 00;22;53;06
—-
This is the standard and a lot of people have accepted this, like you said, that this is their only tool in their tool belt, and they can’t go beyond that. But I think what we’re pushing is that there’s other modalities, there’s other ways of doing it and just thinking differently and I think that in some ways that does challenge the status quo of, you know, how some people run programs.
00;22;53;12 – 00;23;25;04
—-
But I do think that in our opinion, we’re not saying get rid of the mannequins. We’re saying add additional tools to your tool belt to be able to accomplish what you need. Because as a steer, nice patient, what I will say is I don’t want to ever play an unconscious patient in simulation. That is not a good use of my time to lay in a bed with my eyes closed and being an unconscious patient that is not a good use of anybody’s time or energy, because again, then at that point it’s very silly to be giving feedback from an unconscious patient.
00;23;25;04 – 00;23;49;17
—-
The patient’s unconscious. They’re not aware of what’s going on. Like they’re not actually, you know, so that doesn’t make any sense. And then over time, you know, I was a part of a lot of simulations where in the objectives there was no objective about teaching or communication or empathy inside of it. It was very task oriented based off the skills of the students in those situations.
00;23;49;24 – 00;24;04;03
—-
It was not always appropriate to have a C or an ICE patient in those sims because I could sit there for 40 minutes and nobody would speak to me or talk to me because they were getting meds drawn. They were setting up the pumps. They were, you know, they had all of these other things that need to happen.
00;24;04;05 – 00;24;21;08
—-
And part of my feedback to the instructors was, I don’t need they’re not going to talk to me. And that’s okay. Because again, that was kind of my stance is like, they’re not talking to me, but that’s fine because they need to drop meds and that’s not part of the objectives and be like, well, if it’s not a part of the objectives, I don’t think that it makes the most sense that I’m in the room.
00;24;21;14 – 00;24;48;02
—-
I think that a mannequin can fulfill handing them a med and saying, Here’s a side and side effects, here’s what’s going to happen, you know, whatever, whatever. But I don’t need to be there because I’m going to ask me one or two questions, Max, and we’re going to move on. And at that point, being able to have, you know, a mannequin that you’re not paying hourly, that you’re not training, that you’re not doing dress rehearsals with is a better tool for that simulation to meet the objectives that are needed.
00;24;48;04 – 00;25;09;20
—-
So my my, I have a couple of emotional responses to that. But the first the first thing I want to say is the reason that we could even consider in that situation having an ASP is because our pool of ESPs were not being paid. They were actually in a course. So just that’s a caveat because not everybody, not everybody has a kind of an endless pool of ESPs.
00;25;09;20 – 00;25;27;29
—-
Sure. But when I taught I do remember when I talked to that consultant a few years ago with the PS, they and again, I don’t know the extent of it, this was from one person. They did not talk to the ESPs, but their opinion on it was almost a like we have to be an every swim and if we’re not, that’s a problem.
00;25;28;01 – 00;26;05;22
—-
Okay I don’t just take an incentive. Yeah, yeah, yeah. Thank you. I think we need to change it our way too. Should we just go back? Yeah, you can go back. I don’t know where to go back to. I’ll just say we have a number of it. Okay. So I have a number of emotional responses to that. But the one thing I want to say is that people that are listening would say, why in the world would you have that many as PS that you would have the ability to have somebody that’s, you know, in that situation where it’s all skills oriented or, you know, lots of things.
00;26;05;28 – 00;26;25;05
—-
But but we we were teaching a class, we weren’t paying ESP So just to be clear, we did we had to reevaluate our own objectives because we got a little ESP happy. Yeah, but I mean, I will say to you though that with talking to the consultant, she said My ESPs have basically come forward and are like, We need to be a part of every swim.
00;26;25;08 – 00;26;48;13
—-
We’re like almost like and again, this I didn’t talk to the F because I always try to be kind of like we’re taking it as emotional, like a personal attack, that you’re not including us. Like she told me that they said they wanted to be a part of the unconscious Sims and that like basically as the instructor, as the person running the program, she didn’t want to slight them in a way of like saying, yeah, know, you’re not going to be a part of this.
00;26;48;13 – 00;27;14;03
—-
And then it became this like, well, should we be approaching it like So I think sometimes there is this critical element of either the ESPs band together and feel like they need to be a part of every swim where again, you’re not paying specifically for those ESP, So like why not include them? But I do think that coming from someone who again, my background is serious patients, I have a trustee so I can kind of see it from a lot of different sides.
00;27;14;08 – 00;27;38;22
—-
But looking at it objectively, it is looking at it in terms of what is worth my time and energy to put into the training, the preparation, the character and all of these different elements and making sure that it is elevating the same or it’s the right tool in the toolbox, right to be able to include it. And I do think that sometimes people lean more towards using mannequins than they do serious patients.
00;27;38;22 – 00;27;55;07
—-
I think that’s the natural lean. But I do think sometimes we can lean water using sterilized patients when the mannequin might be appropriate, especially based off the objectives. And I think sometimes it does. You have to get a little bit removed because I think we kind of favor one tool or another. I do think that can happen. Absolutely.
00;27;55;10 – 00;28;11;19
—-
But trying to look at it objectively and I will just say from one sterilized patient to others are nice patients. It’s not a personal slight if you’re not used in every swim, it’s okay to have other swims that you are not a part of. And sometimes maybe it’s better for you to be the family member of that unconscious.
00;28;11;21 – 00;28;30;11
—-
That’s what I was going to say. Or, you know, maybe it’s better that you are, you know, like adding. But sometimes, especially in terms of like thinking about med administration or getting the pump set up and things like that, sometimes your level of learners aren’t also ready to deal with an upset family member or an upset patient or whatever it is.
00;28;30;11 – 00;28;53;18
—-
So just sticking that objective in there, sometimes now you’re making it too hard because you’re asking them to do all of these different components, plus now dealing with that live person. Yeah, I mean, my own personal experience is that when you get to the point of doing some of those med surge swims, that they if they are in a clinical experience, they are going to have family members that are going to be asking them questions.
00;28;53;18 – 00;29;12;05
—-
So if you’re talking fundamentals or you’re talking to some of the very early on before they get into a lot of the clinical experiences, I can understand that. But but at the end of the day, being able to talk to concerned family members is a skill that needs to be developed. So I would it has to be a part of the objectives.
00;29;12;05 – 00;29;32;28
—-
I think that’s where things can get lost, is that if it’s not added into the objectives and you’re just now like and we have a family member, let’s ask Suzy down the hall to come in and play that family member. And it’s not a part of the objectives. The pushback that I always got was, well, we don’t really care about that in the sense or like if they don’t talk to you, it’s fine because it’s not really an objective.
00;29;32;28 – 00;29;49;16
—-
And I think that’s the part that it’s just like if you’re going to include that and I agree with you that if they are going in the clinical setting, they will be expected to answer questions. They will be expected to interact with people and need to learn how to do both things at the same time. But it’s got to be in the objectives.
00;29;49;19 – 00;30;21;05
—-
No, I agree with you on that. But but from as a simulation, it’s basically like I would always include it in its objectives. That’s just and it just may be my my own personal bent, but it is just seeing how realistic or how, you know, how sometimes that can really mess you up. I mean, there’s been times where, you know, they’ve been doing clinical rounds on a patient and it’s a woman in her, you know, let’s say sixties and next to her is sitting a man in their sixties.
00;30;21;07 – 00;30;40;22
—-
And they the clinical team is going all through this patient’s history, yadda, yadda, yadda. And it’s the neighbor. Yeah. And it’s not it’s not her husband or, you know, brother or whatever. Like, nobody’s taking the time to check that kind of stuff out. So again, it’s just really important that they understand the dynamics and how you address that.
00;30;40;24 – 00;31;03;14
—-
You know, there’s a million things and there’s a lot to learn in health care, but it is something where I do think there’s a time and a place. And no matter what, if it’s not in the objectives, if there’s no communication, no education, no assessments that are necessary, you know, that was one of the things when we were at the New England Swim Summit that the individual from Yale said, I can’t remember name, I’m so sorry.
00;31;03;14 – 00;31;28;17
—-
But she said, you know, when you need non-verbal reactions and you need, you know, the patient to be demonstrating certain things, especially assessment, like think of like stroke patient and they need a slurred speech and, you know, deficit in their, you know, weakness and in their one side versus the other. That’s all stuff that is way more approachable or things that were are emotional where like they’re doing some stuff with pastoral care there.
00;31;28;17 – 00;31;52;08
—-
And so having a mannequin is just not the same. You know, it doesn’t have the same energy in the room. So but I will say that for mannequin based simulation, anything that is unconscious that doesn’t that is very highly task focused does really warrant a mannequin. The other big one is pediatrics, right? That’s kind of another big place where mannequin simulation can be appropriate.
00;31;52;08 – 00;32;09;27
—-
So on the flip side of that, I think that there’s also the limitations that come with incorporating mannequins in terms of, you know, I didn’t realize this, but in their user manual, it says that they should not be moved out of the bed once they’re placed in the bed and they’ve had some personal experience with breaking a board.
00;32;09;29 – 00;32;33;19
—-
Yeah, I think that it was like once I heard that, that that was in there, use me. I was like, yeah, that tracks because we were not. I agree experiences with that. But I do think that there’s and as a caveat, we don’t know every single one. We were we, we just know that the ones that yeah there’s sure there’s someone’s right but in those terms I think that that does make it very complicated as a simulation is where you are not able or you’re not supposed to be moving them out of the beds.
00;32;33;21 – 00;32;53;15
—-
There’s the obvious limitation where the patient can’t get out of the bed and can’t move. I think that there’s been a lot of energy and effort in terms of trying to make mannequins have more human features or elements like again, they’ve been working so hard on making this mean I can be able to move its hand up to be able to do a handshake.
00;32;53;18 – 00;33;13;13
—-
And when we talked to Krystal for you, she was like, I’ve done that. A conference is every year, you say, and it’s not the same thing as shaking somebody’s hand, right? So I do think that there will be these limitations that happen, you know, making mannequins cry and things like that. It’s fine until the mannequin breaks and then it can no longer cry anymore.
00;33;13;13 – 00;33;38;02
—-
Right. And then now what do you do for that? Same because you don’t have that element. But I do think that there’s the appropriate times and places. But I do think that those physical limitations is it is still not the human body, it is still not a human person. And I do think that you’re still going to struggle if you’re solely relying on the technology to make the facial expressions or to show sepsis and the like.
00;33;38;02 – 00;33;57;16
—-
I just think it’s you’re going to have a harder time when it is that mannequin. Nonverbal communication is what I think the 80 or 90%. Yeah. And so and that is always going to be a limitation because they can put so much money and effort into making those mannequins more and more realistic. But it is still going to always it’s going to be human.
00;33;57;16 – 00;34;14;07
—-
It’s just not you’re just always going to you’re always going to lack that. And I think that really impacts, you know, what your objectives are, what you want. And quite honestly, the more technology they put into it, the more expensive it is, right? There’s a lot of research and development that goes into it. So, you know, yeah, how much can the how much can you bear as far as.
00;34;14;09 – 00;34;41;07
—-
Yeah. Cost. Absolutely. And then looking at the pediatric side, this is a more controversial topic inside of simulation. Even if you look at it from, you know, internationally, Australia has a lot of literature that’s come out. The UK has a had a lot of literature come out. The U.S., I don’t think has much, but there’s a lot of opinions here in the U.S. and I would say that this is one that I feel a little a little torn on.
00;34;41;07 – 00;35;00;04
—-
And I think it definitely depends on the situation you’re in. But I’ve heard several times people say, well, if you’re doing VR tricks, you’d have to use a mannequin. There’s no other choice. And in Australia, one of the SIM centers that I visited in Melbourne, baby had a lot of pediatric surgeries. Patients, they had a whole pool.
00;35;00;07 – 00;35;19;21
—-
It was something that like they were very confident when that was what they did was that they had children. I think it was from about 5 to 15. They had a lot of pool and they were all child actors. But the important part here that I think is often overlooked is there is so much energy and effort that goes into having these children.
00;35;19;21 – 00;35;52;20
—-
And I was going to say, like, if you think about like a movie set, if you’re going to film a movie now with, children, there are so many components from legalese to, you know, how long they can work, child labor laws, you know, the the emotional toll that it can take. But they have someone designated to their child stare at ICE patients that is solely there for their, you know, to check for the child labor laws, to check for the psychological and physical safety to manage the parents of the children.
00;35;52;22 – 00;36;14;20
—-
And it is built into it. And when you talk to them, when I was touring their center, it’s like they talk about like, yeah, this is the easy. Like, of course, yeah, you just hire someone and they manage it and like, yeah, no, What? What do you mean? And I think that sometimes that is not necessarily realistic of all simulation programs to think that they can just hire someone to manage, you know, just their pediatric sims.
00;36;14;20 – 00;36;37;21
—-
You know, it’s kind of like the council in on hiring someone who just means your your maternity systems or your bed search sense. So it feels very complicated. But I think here in the U.S., a lot of people just steer clear of it. Or on the flip side, which personally I think is more dangerous, is a lot of people will just bring in their young children, put them in a bed and be like they’re the they’re the patient for today.
00;36;37;27 – 00;36;56;19
—-
And I think that having children who are, you know, their parent works in shame or whatever it is. Now, again, speaking as someone who personally went through this, I was 16, though, and I had already had acting experience and I knew what I was getting into. I was given training. I went through the full gamut of what need to happen, but I was 16.
00;36;56;22 – 00;37;18;00
—-
I think it’s very different when you bring in a five year old putting them in a hospital gown, telling them that they’re sick and then expecting them to run through them. And I think that that’s the part that gets dangerous is that if we are just kind of viewing this as, it’s no big deal, we’ll just throw somebody in that can be very traumatic to children for not being able to separate the realities.
00;37;18;08 – 00;37;46;06
—-
So I think that there’s a lot of different angles here. I think the positives of obviously having a pediatric mannequin is that you don’t have to worry about including a live person. But as a serious patient who’s done a lot in terms of being the mom in the room, it does feel very awkward to have this child that you’re supposed to love and, you know, and all of this and you can hear the mechanics of the head turning.
00;37;46;11 – 00;38;08;19
—-
You can hear the mechanics of it, you know, moving it. It’s it’s a little creepy slow, Chucky doll kind of thing. Like it’s scary. So I do think that there’s elements of being aware of the psychological safety of having a real human, having the limitations of the technology of the mannequin. And then I think finding the appropriate middle ground.
00;38;08;25 – 00;38;25;09
—-
And I do think bringing in 13 year olds, 14 year olds or even having 16 year old to look younger, playing the role of a 13 year old and things like that, all of those things are possible. I played young patients all the time when I was 16 because I could get away with it. And having that I think is also an added benefit.
00;38;25;15 – 00;38;46;13
—-
But when you’re talking five, six, you know, to the thing that you’re going to be able to bring in a real child, I think that it’s just considering the potential damage for the potential reward in weighing that. Yeah. I mean, I think obviously they have very sophisticated system and they have, you know, whatever site that you’re referring to.
00;38;46;20 – 00;39;16;12
—-
I know there’s a site in Utah that does along with pediatrics in space, it’s almost like I remember Bethany, my other daughter, she was talking about in theater, if they have a sex scene or have some kind of scene, there’s an intimacy coordinator or something. It’s the same kind of idea where you definitely need somebody that’s really I think that that’s the part that I would want to emphasize here, is anyone who is thinking about bringing in like understand that people don’t just take children and plop them into a movie and say, okay, go ahead.
00;39;16;18 – 00;39;35;23
—-
Like, that’s not there’s so much that goes behind the scenes. There’s so much additional work that happens. There’s so much technical pieces that go into it, too. Again, I don’t think that that always happen. If you, you know, think about like Wizard of Oz things, I think they’re like happened in those days that we’re not kosher. But in today’s day and age, there’s so much behind the scenes that we don’t see.
00;39;35;23 – 00;39;53;27
—-
And I think sometimes it’s just this element of like, well, they do in the movies, why can’t we do it here and just understand that there’s a lot that goes behind that. And it doesn’t mean that it’s impossible, but it means that there’s a lot of pieces to it. And I think sometimes it’s just better to use the mannequin to avoid all of these additional components that would be expected of you.
00;39;53;27 – 00;40;18;11
—-
Now that you’re kind of taking this on. And quite honestly, the same way that Ashby put forward the sorts of best practices, they’re nice patients. I do think that if pediatric patients started to become more prevalent, I think there would be different standards. Yeah, if you’re under 18, think that there would be a different level of expectation and code of conduct and code of conduct in a way of approaching it when they are under 16 years old.
00;40;18;11 – 00;40;39;06
—-
But I think I know ask be released one for the people that do the genital teaching exams. So there’s a specialized thing that so I could see the same kind of yeah I think I can see it passing over into the pediatrics as well too. That’s a good point. Yeah. All right. So moving on to VR and AR, so this is really, I guess, yeah, we kind of killed s piece of mannequins at the same time.
00;40;39;06 – 00;40;55;15
—-
So we really kind of approach that. It’s kind of a double edged sword. I do think that in a way there is there can be a lot of harmony there of including both of them in a hybrid situation. So I do think that there’s a lot of ways of being able to merge those two together and figuring out what’s appropriate between the two.
00;40;55;15 – 00;41;25;08
—-
But yeah, no, I agree. I think we chat about both of them. So going on to air VR, I know that you recently had a conversation with Dawn from Oxford Medical Oxford Medical Simulation, which really focuses on the AR VR side of things. So do you want to chat a little bit about what that conversation was about? Yeah, And I think also, you know, I’ve talked to several people about AR VR because it is kind of the up and coming and everyone’s, you know, looking at at the technology and watching it develop over time, which is really kind of cool.
00;41;25;10 – 00;41;50;14
—-
But the the other really big impactful conversation that I had her was actually like a seminar that I attended. So we were I was presenting at the Mayo Clinic, but one of the other individuals, his name was his first name was Eric. I can’t remember his last name, but he is definitely an expert. He did his Ph.D. on VR and he actually came up with a kind of a whole appropriateness of where AR VR can be used.
00;41;50;14 – 00;42;21;18
—-
And it was very similar to my conversation with Don as well. But AR VR is a really great preparatory work. So if you think about, you know, like when you go over, you go to the same conferences, they’re, you know, doing operating room things or even like caesarean sections and things along those lines. And so preparing the room or, you know, not every not every sim center has an O.R. that they can practice in with all of the different trays and all the different things.
00;42;21;18 – 00;42;45;16
—-
So having an AR VR system or they can, you know, move the things again, I don’t I’m not an owner, so I don’t know very much about it, but just that they can function within that role based off of what you’re trying to teach them within their program. And preparing them is really a great preparatory piece. He’s he talked a lot about, you know, if you actually have the the actual tools that they would be using.
00;42;45;16 – 00;43;06;22
—-
So if you think of the Da Vinci surgical robot or I don’t know exactly how what they call but The Da Vinci Tool, you know, having the someone who’s getting ready to do a surgery for the first time, practicing with actually using that device the way that it’s supposed to be. And there’s like a lot of stuff out now with endoscopy or colonoscopy or whatever it is.
00;43;06;22 – 00;43;29;29
—-
So they’re actually like using the the actual physical pieces of this, but visualizing something different. There’s a lot of benefit to that, right? Where you’re preparing them for a difficult or complex scalar task. And then the other place where they talk a lot about where it’s really, really good, both at both John and Eric talked about where it’s really good is warming up.
00;43;30;06 – 00;43;55;28
—-
So if you think of a surgeon who’s maybe they’ve done use The Da Vinci Tool for this type of surgery 100 times. So, you know, heart bypass surgery. But this morning before the first surgery, they go in an hour early and practice on The Da Vinci Simulator. They’re warming up. You know, it’s kind of like a tennis player, like just, you know, let’s just go through and you can put those those high, high stakes, low volume simulations, right.
00;43;55;28 – 00;44;26;09
—-
Where, you know, an artery gets nicked or something happens and you can, you know, create that visually in within the again, I don’t the Oculus devices, when we were at GW, Crystal had just purchased some AR VR, and I asked her about people getting like that motion sickness because that that’s something that’s related with the VR. So AR is usually not having that motion sickness because you’re again, just augmenting the reality of having something that comes up at the VR is the full encapsulation where you are, right?
00;44;26;09 – 00;44;44;09
—-
And so that is more common with the VR. Yeah, but what she said is that they can projected on the screen, which at that point I assume then it is more like augmented reality where you’re not seeing it through the Oculus, but you’re seeing that the augmented reality is more supposed to be like anything like Pokemon Go where you’re seeing it through the screen.
00;44;44;09 – 00;45;04;02
—-
And so one thing is coming up and so it’s just kind of looking at like, so if you’re looking at it through your phone and it looks like there’s a Pokemon character running around the room, but it’s just that one element. So with a projected, I don’t really know what that term would be. I don’t know what they call it, but again, with the virtual reality, it’s just supposed to be that it’s more of the whole Yeah, setting.
00;45;04;02 – 00;45;35;09
—-
But again, there has been a lot of discussion about whether people get motion sick with it, so they have to come up with an alternative for that. Yeah. Dawn also mentioned within her particular product is that they have the the ability now to do multi patient simulations. So you know if you think of like a you have a five patient assignment now and you’re individual because like typically in Sam it’s two, three or four people that are going in there now you’re by yourself and you’re managing all of this.
00;45;35;09 – 00;45;52;26
—-
It gives more of a reality of what’s going to be It’s going to be like when they’re actually doing care again. I think it’s less I think that that’s like the appropriate first step in that kind of what you’re term. I was like that warm up is throwing them into a room with mannequins and serious patients and kind of like, you know, a triage type of situation.
00;45;52;28 – 00;46;13;18
—-
If they started with doing that in a VR setting of learning of how to triage and learning how to prioritize and all of these different elements, that’s also going to be that kind of first step. And then it’s like, okay, you’re practicing now in this virtual setting where it’s a little lower stakes. Now we’re going to be able to put you in a scenario where, again, you maybe you have multiple mannequin, multiple series patients, things like that.
00;46;13;24 – 00;46;37;24
—-
Now let’s use those same skills that we had been practicing in that VR world. Now, the only struggle with that is that it’s very typically, typically pretty difficult to get five patients in a similar right to choose probably max. And typically because of time you want two or three people in there. So you might have one. That’s the tech and one that’s a charge nurse and one’s that, you know, the the primary nurse or something.
00;46;37;24 – 00;47;16;25
—-
And you can recreate it that way. But where VR shines is they kind of have their own individual performance that they can check on. But there are limitations. The technology isn’t quite there yet, far as tactile feel. And you know, the graphics, yeah, there’s there’s some limitations with that but but it is again that’s really where if you look at what Eric’s work at, I should probably know his last name and I don’t I apologize but it really is focused on if you think of preparatory before they’re actually doing clinical care or they’re doing simulations and then also with reinforcement afterwards.
00;47;16;25 – 00;47;48;01
—-
So if you think of if they don’t typically get trained patients on a unit and now they’re going to get a patient, maybe there’s some eventually there might be something that they could use as a warm up or something like My difficulty with the air VR is in some ways I think part of it is the marketing of it, but I have a hard time when it’s being marketed as this is a cheaper, faster way of doing them because they advertise is you don’t have to have someone who watches, You don’t have an instructor who watches the same, you don’t have to have to do a debriefing.
00;47;48;08 – 00;48;08;25
—-
And basically this is all a self-contained thing. And they do a cost comparison between if you were to purchase a mannequin, need a facilitator, here’s the cost that here’s what the cost would be with VR without needing that. And I do think that trying to compare those two things as here’s a cheaper, faster way of doing it, in my mind, it comes back to that like silver bullet.
00;48;08;25 – 00;48;24;17
—-
There’s no easy way to just make this where it’s going to be, you know, no money and super fast to get through because I don’t think the students are getting that same experience if they don’t have a facilitator. The whole point is, you know, we know that they do that they have 80% of their learning happens in the debriefing.
00;48;24;23 – 00;48;47;23
—-
So we just completely, entirely skipped that step. I don’t think they’re going to gain the same knowledge. I agree with what you said in terms of a warm up and also kind of like solidifying concepts and things like that. And I think those are great technologies to use that, but I don’t think that it can be compared apples to apples in terms of a full blown SEM, you know, with a facilitator with other peers involved.
00;48;47;23 – 00;49;03;14
—-
And, you know, again, learning from each other and then going into that process because I think it really does in some ways when it is compared apples to apples, I think in some ways it does cheapen what we do in SEM because it’s saying, well, why do you even need a facilitator? Let’s just move. Why even have a similarity?
00;49;03;15 – 00;49;27;24
—-
Let’s just move all into this and then call it a day because it’s cheaper and faster. And I think there’s pieces for it. And like I said at the beginning of the episode, I think there’s a place for all modalities in terms of what their strengths and weaknesses are, but I really don’t like to compare it apples to apples to others, because I do think that then you’re you’re lacking the facilitator knowledge, which I think is also a huge piece of it.
00;49;27;27 – 00;49;46;10
—-
100%, I would agree with you. And that kind of goes back to the whole psychological safety, you know, all the different aspects. If they don’t know what they did incorrectly or if they’re not, you know, if they’re not being guided by a professional, that that does lead to some some challenges. You know, there’s ways that they that they have looked at debriefing.
00;49;46;10 – 00;50;05;26
—-
And I talked to Don about that as well. But I do think that there is huge benefit to, you know, the idea that we’re going to go through a debrief, utilizing a debriefing model where they’ve just gone through the simulation. Now let’s talk about it. Yeah. In reframing their thoughts and, you know, allowing them to see where potentially they have room for growth or opportunity.
00;50;05;26 – 00;50;29;22
—-
And I think that at the end of the day, you know, the idea of reducing burnout, you know, preparing them the way that they need to be prepared for clinical, it is going to involve all of the modalities. And at the end of the day, there’s no silver bullet, as you mentioned. There’s no panacea. And you have to look at your objectives and you have to look at your level of learner and you have to make the best decision with the modalities that you have at your fingertips.
00;50;29;22 – 00;51;00;29
—-
Yeah, You know, I think right now people that are kind of looking at that newer technology are early adopters, you know, and they’re, you know, there’s a that’s not available in every every simulation center, but it is something that is out there now as an option. You know, we we probably, I don’t know, six or seven years ago now, we visited California Baptist for the first time and they had an immersive room where their students techs put this amazing, you know, like it was like a rain forest when we went in.
00;51;01;07 – 00;51;25;14
—-
It was just stunning. Yeah, but that and that’s the part to me that that’s where I struggle with, is they have these immersive rooms at Cal Baptist, which again, it is not VR, you’re not wearing goggles, you don’t have any special technology. It’s projectors on the wall. It’s different sound equipment. They’ve used a lot of tactile things like putting mulch on the floor so that when you’re walking, it doesn’t feel like you’re just walking across a smooth surface to make it feel like you’re outdoors.
00;51;25;17 – 00;51;41;10
—-
I don’t necessarily know how they would involve that, but then you have the immersive rooms that are sold by Echo, where it’s kind of that blow up room with just the projectors. And then me, I’m like, Well, those two aren’t the same thing because there’s one that has the mulch on the floor. I like all the different components.
00;51;41;15 – 00;51;59;25
—-
One that’s kind of more of just a projector screen in a room. And I think that that is something that as a newer industry, you know, for health care said that we are still figuring it out. We’re not, you know, you know, automotives like. Right. We haven’t been around for hundreds of years. We’re still figuring out these definitions and we’re still figuring out where do things fit and where do they go.
00;51;59;25 – 00;52;21;05
—-
And I think some people disagree. I think some people think, you know, this belongs with this or this is the same thing. And again, I think that those types of technologies, I do think more people will move towards these rooms again. And theater, you know, we call them black box theaters where they can really be moved and changed and all of these different things to meet the needs of what you know, that theater wants to do.
00;52;21;07 – 00;52;41;27
—-
And I do see simulation moving towards that direction. I think more and more people are starting to include that, but it really doesn’t have a clear definition or a clear modality at this point of what should be considered. I don’t know if it’d be even considered a modality, maybe a just be considered an environment, I don’t know. But it is really interesting to see how things grow and change over time.
00;52;42;01 – 00;53;03;03
—-
You know, for us, we were very to see that there is a gap in the market of needing wearable simulators. So really that was taking the benefits of the TAFEs trainers and, you know, the technology, the mannequins and then the human element of the series patients. And then being able to merge that with these wearable products that were designed to be worn.
00;53;03;06 – 00;53;27;13
—-
And I have haptic feedback inside to. Q That’s your nice patient. And there are different ones that we would also consider wearable simulators. So if you think of the Cup suit, maybe you think of even telescope, things like that. There are other ones that the telescope is just a stethoscope. It’s khadi onyx it has a that that the shirt breaking that those pieces like ventral scope has with the augmented you know stethoscope.
00;53;27;16 – 00;53;46;16
—-
I don’t really know where that fits. Mom and Natalie, it’s a wearable, but I wouldn’t necessarily consider it a simulator because there’s really not any technology that’s inside of the product. So there are still kind of these ideas called outliers, where we’ve really coined the term wearable simulators to define something that is wearable and has technology built in.
00;53;46;22 – 00;54;10;16
—-
But there are other wearables that don’t have technology built in, and those really kind of fit in a no man’s land at this point of trying to figure out where these definitions live and thrive and things like that. And to create new categories for every product that pops up. I don’t think it’s necessarily feasible, but when you do start to see it more and more, it does start to expect, you know, some sort of category.
00;54;10;16 – 00;54;32;29
—-
We did our best to attempt to categorize them into defining excellence in the simulation chapter because there aren’t it. It’s such a broad variety, so broad. But even if you think of like simulated thermometers and blood pressure cuffs and pulse ox is like, where do they fit? Right? Yeah, they’re not really test drainer, but we covered it in the test trainers chapter.
00;54;32;29 – 00;54;55;05
—-
And again, lots of really good uses use cases that we offer to that in that chapter. So again, I encourage you to read it if you have it or you know, check it out of your library if you if you can get the interlibrary loan. But I think that at the end of the day, our main message is there’s multiple modalities and multiple opportunities for using tools in your tool belt.
00;54;55;07 – 00;55;24;10
—-
If you don’t have the modality where that particular stimulation would fit best, consider, modify, saying the objectives of the simulation to fit in with what the tools that you have within your tool belt. And the other thing that I think we’ve talked a lot about is hybrid sim. And I understand that that may not always be the easiest based off of what your limitations are, but I do think hybrid SIM and merging a lot of these modalities together to create an authentic experience is usually always going to be the ideal.
00;55;24;10 – 00;55;43;09
—-
Is it always possible? Probably not. But I do think in terms of being able to merge multiple modalities is often and I think that’s where we we naturally lean is usually in the hybrid because usually it’s like, well, I want this piece and I want this, but let’s figure it out together. Let’s get started, let’s make it. And I think that’s great.
00;55;43;12 – 00;56;04;11
—-
But I do think that in some ways it is people kind of relooking at their sims and making sure that whatever those objectives are and whatever they want it, what they want the outcomes to be is really assessing the tools that they have. The other thing I just want to do a quick shout out before we end here is there is usually times that we go through people, some labs and we’ll do tours.
00;56;04;13 – 00;56;23;29
—-
And so often I hear people say, that stuff has been on our shelves for years and we don’t touch it. We don’t use it. And those are the kinds of things that I really encourage people when you’re coming into a new SIM center or just refreshing things, look at the tools you have because I think there’s lot of times that things are just on the shelf and you don’t even realize you have it.
00;56;24;06 – 00;56;46;14
—-
And maybe you started a new SIM a few years ago and you didn’t realize you had this. But then now you can reassess and see, this really is the best piece. Those are the types. I just encourage everyone, like dust the stuff off your shelves, Take a look at it. Figure out really what it is and challenge yourself to make sure your Sims are really using the proper tools that you have to get the most out of them.
00;56;46;16 – 00;57;10;24
—-
My other word of advice would just be there’s a lot of consultants in the world of SEM and a lot of people who are willing to kind of just chat about things in terms of what’s out there, chat with some people about what other tools they have in their tool belt of what they use at their SEM lab, because I think a lot of times we’re not great at knowing everything that’s in the industry, especially if we don’t have budget to go to IMH and a Naxal and all these other places.
00;57;11;00 – 00;57;29;08
—-
If you’re not able to really get out there, you don’t really know what you have available. Yeah, but talking to some people in your area or your, your, your team or, you know, people who are local to you, if you have a SIM group or something like that, there can be a lot of understanding that there are a lot more things out there and kind of keep an open mind to what that could be.
00;57;29;14 – 00;57;51;04
—-
Yeah, I would say if you’re new to simulation, do a few tours. yeah, do a few tours, you know, spend. You don’t have to spend any money just contact a couple of the other SIM centers in your area and go see what they have. We’ve done tours all over the country and there are some amazing SIM centers and there’s a more humble SIM centers that are still doing amazing things.
00;57;51;04 – 00;58;04;21
—-
So I take a minute to look around and get really creative. I think that that’s the other piece there is there’s a lot of people get really creative with what they do to meet the objectives that they have. I think that’s in SIM, we are able to really get our IT exactly. We’re able to really figure it out.
00;58;04;23 – 00;58;51;02
—-
And again, we appreciate you guys listening. I’m sure that we could have talked a lot more about different modalities. There’s a lot more we could have covered here. But again, we want to just keep this kind of concise, high level, keep it simple. So we appreciate you listening. Any questions? Leave them in the comments and we’ll see you guys soon.